

















Current COVID-19 Situation
According to the Nepal Ministry of Health, as of November 11, 2020 Nepal has reported 202,329 confirmed cases and 1,174 confirmed deaths due to COVID-19. Nepal currently ranks 34th globally and 11th in Asia in the absolute number of confirmed cases.

On per capita basis Nepal now has surpassed India in the cumulative number of cases since the start of the pandemic: 6,856 in Nepal compared to 6,226 case per 1,000,000 population. In the past month, the new infections rates in Nepal have been 2-3 times the rate observed in India. On November 11, 2020 the 7-day average of new infections rate in Nepal was 99 cases per 1,000,000 population while in India it was 33 per 1,000,000 population. These statistics indicate the severity of the ongoing epidemic in the country.

Evolution of COVID-19 in Nepal
Since the beginning of October, the epidemic in Nepal has been growing rapidly and now concentrated in the Kathmandu Valley and densely populated districts with urban areas in Eastern and Central Terai. In fact, 57% of all cases in Nepal have been reported since the beginning of October.
Although there seems to be a decline in the number of new cases in the past two weeks, the observed decline is likely an artifact of the decline in testing and reporting due to Dashain holidays. In fact, it would not be surprising to see another rapid increase in the number of cases in the next two weeks as a result of increased transmission during Dashain holiday travels and increase testing and reporting.
With 1,174 total confirmed reported COVID-19 deaths the observed case fatality rate (CFR) in Nepal currently stands at 0.58%. The observed CFR rate is substantially lower than that observed globally including India which has a CFR of 1.5%. The possible explanations of the lower observed CFR in Nepal may include the younger population in the country, infections occurring in younger and healthy individuals, lower rates of comorbidities such as obesity, hypertension, and diabetes in individuals currently at a higher risk of COVID-19 infections, and undercounting of COVID-19 deaths. It should be noted that 50% of the total confirmed deaths in have occurred since October 1, 2020. As the number of infections rise, the number of deaths will likely continue to increase in the country.
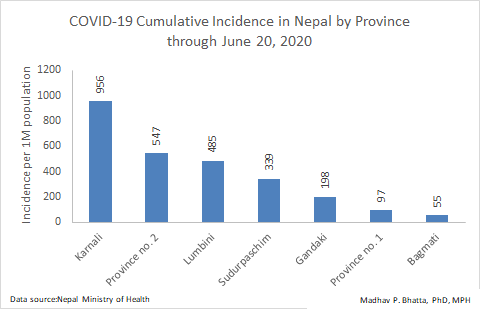
During the first phase of the COVID-19 epidemic in Nepal in June, cases of primarily among the migrant workers returning from India and infections that were occurring within poorly managed quarantine facilities housing these workers. Thus, the highest incidence of cases in were reported in Karnali, Province No. 2, Lumbini, and Sudurpaschim Province, which had large migrant workers returning from India after the lockdown there. Bagmati province, which includes densely populated Kathmandu valley had a low rate of transmission as a result of the national lockdown during that time. Since most of the migrant workers hailed from rural villages in the four highest incidence provinces—and low-density hill regions in Karnali and Sudurpaschim Provinces– it appears that the infections were self-limiting these the provinces. While the infections in these four provinces have risen since June, the increase through October does not appear to be substantial; it ranged from about 5-times in Karnali to 12-times in Sudurpaschim Province.
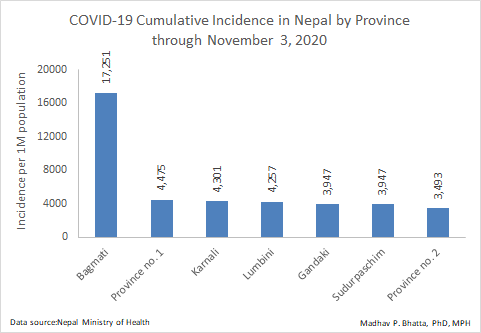
Bagmati, Province No. 1, and Gandaki Provinces had the lowest incidence of COVID-19 in Nepal in June but since then the rates in these Provinces have dramatically increased. In fact, the epidemic since June has been primarily driven by the dramatic rise in the number of cases in these three provinces, but especially in Kathmandu Valley in Bagmati. The incidence rate of COVID-19 in Bagmati Province as of November 3, 2020 was 17,251 cases per 1 million population—4 to 5 times higher than the other provinces. The increase in the number rate of COVID-19 followed the reopening of the country in June and July. While the country was reopened, it appears that there were limited, if any, public health mitigation measures that were developed and implemented post-reopening, especially in densely populated urban center of the Kathmandu. As a result, Kathmandu Valley is seeing a massive surge in cases.
Likely Winter Trajectory of the Epidemic
As the winter season approaches there are several factors that could further exacerbate the COVID-19 epidemic in Nepal. The increased risk and upward trend in infection are especially worrisome in the Kathmandu valley and other urban areas. First, the current transmission rate ongoing into the winter months is high. Second, the movement of people within the country for Dashain and Tihar holidays is likely to increase the geographic spread of the virus and amplify the virus transmission in the country. Third, colder winter weather generally favors the virus transmission as people are more likely spent more time in indoor enclosed spaces and the cold dry facilitates airborne transmission. Fourth, air pollution in the Indian sub-continent including Nepal peaks during the winter months, which increases the vulnerability of the respiratory tract to infections. Fifth, after over 8 months of dealing with the pandemic, people are “pandemic fatigued” and thus may start laxing on the mitigation measure of public facial covering, social distancing, limiting gatherings, and good hand hygiene. Sixth, there are a lot of misinformation and false information circulating around about the pandemic, which can play negative role in controlling the pandemic.
While the COVID-19 infection rates in rural hill communities with limited populations mobility may continue to remain low and self-limiting, the pandemic in urban centers and low-land districts in Nepal is likely to continue to increase in the months ahead. The public health system in Nepal at the national or local levels does not appears have the capacity of developing and implementing targeted mitigation measures to control the epidemic. The ‘Lockdown’ approach taken previously is not a tenable long-term strategy in absence of any other measures. The healthcare system is not capable of providing clinical services to serious cases needing medical intervention. With the increasing COVID-19 infections, the deaths will likely increase as well but due to lack of effective system of ascertain of deaths, it will likely be challenging to know the true extent of the problem. Effectively communicating to the public and the public adopting the known public health mitigation measures to the spread of COVID-19 may be the only viable option for Nepal avoiding a long and painful winter.
Madhav P. Bhatta is a Professor of Epidemiology and Global Health at Kent State University College of Public Health. He received his Bachelor’s degree from the University of Pennsylvania and Masters of Public Health (Epidemiology and International Health) and PhD (Epidemiology) from the University of Alabama at Birmingham. He was born and raised in Nepal.
https://www.facebook.com/madhav.bhatta.90
https://www.linkedin.com/in/madhav-bhatta-093b3314/